Introduction
Indoor dampness and mold problems are universal and thus are potentially of major public health importance (1-11). Such problems have been surprisingly common in countries with cold climates, such as Finland, Sweden, and Norway (4,5,9,11). The major reasons for the high frequency of such problems in cold climates may be insufficient maintenance of the buildings and construction of tight buildings to conserve energy accompanied by inadequate ventilation. Residential dampness problems have been related to increased risk of asthma and asthma-related symptoms in children (1,2,4,6,8,12-15) and in adults (7,9,13,15-20). However, we did not identify any epidemiologic study of workplace indoor dampness and mold problems and asthma, and only four studies have evaluated potential effects of such problems on wheezing (5,10,21,22). These studies were carried out in either daycare centers or offices. Most of the studies among adults were cross-sectional or prevalent case-control studies in design, and almost all of them based the diagnosis of asthma or asthma-related symptoms on self-report in questionnaires or interviews.
The objective of our study was to assess the role of dampness problems and molds at work and at home in the development of asthma in working-age population. We recruited incident cases of asthma, the diagnosis being verified with clinical examinations. We also evaluated some personal characteristics, such as age, sex, and smoking, as potential indicators of sensitivity to the adverse effects of dampness problems.
Methods
Study Design
This study was a population-based incident case-control study. The source population consisted of adults 21-63 years old living in the Pirkanmaa Hospital district. This district is a geographically defined administrative area in South Finland with a population of 440,913 inhabitants in 1997. Our goal was to recruit all the new cases of asthma in the source population during the study. We selected controls randomly from the source population based on 1997 census data. The ethics committees of the Finnish Institute of Occupational Health and the Tampere University Hospital approved the study.
Definition and Selection of Cases
We systematically recruited all the new cases of asthma, first in the city of Tampere beginning on 15 September 1997, and then in the whole Pirkanmaa Hospital district from 10 March 1998 to 31 March 2000. We recruited patients at all health care facilities diagnosing asthma, including the Department of Pulmonary Medicine at the Tampere University Hospital, offices of the private-practicing pulmonary physicians in the region, and public health care centers. As an additional route of case selection, the National Social Insurance Institution of Finland invited all patients to participate whose reimbursement rights for asthma medication began during the period 1 September 1997 through 1 May 1999 and who had not yet participated.
We applied the following diagnostic criteria for asthma: a) history of at least one asthmalike symptom (prolonged cough, wheezing, attacks of or exercise-induced dyspnea, or nocturnal cough or wheezing) and b) demonstration of reversibility in airway obstruction in lung function investigations. Table 1 presents lung function findings accepted to demonstrate reversibility. These diagnostic procedures correspond to the recommendations of the National Asthma Program in Finland (23).
We selected as cases all the confirmed cases of asthma fulfilling the general eligibility criteria. A total of 362 cases (response rate, 90%) participated through the health care system, and 159 cases participated through the National Social Insurance Institution (response rate, 78%), totaling 521 cases overall.
Selection of Controls
We randomly selected the controls from the source population using the national population registry, which has full coverage of the population. We applied the general eligibility criteria for controls. After up to three invitation letters and phone calls, 1,016 participated in the study (response rate, 67% of total invited population, or 80% of those who had a phone number in the Pirkanmaa area). Previous or current asthma was reported by 76 (7.5%); six persons were older than 63 years, and two returned incomplete questionnaires. After excluding these persons, our study population included 932 controls.
Exposure Assessment
We based exposure assessment on questionnaire information about water damage, damp stains and other marks of structural dampness, visible mold, and mold odor, both at home and indoors at work (4,5). For water damage, damp stains, and visible mold, we asked for information about their occurrence during the past year, 1-3 years before, or > 3 years before. For mold odor, we asked the subject about occurrence during the past year and to indicate if such odor appeared almost daily, 1-3 days a week, 1-3 days a month, < 1 day a month, or never.
Data Collection
At the Tampere University Hospital, we recruited cases at their first visit for suspected asthma, and we verified the diagnosis in clinical examinations. At the other health care facilities, cases were recruited immediately when their asthma diagnosis was verified. We applied the same protocol for diagnosing asthma at all health care facilities. The National Social Insurance Institution invited the cases 6 months to 2 years after their diagnosis was established. For these patients, we confirmed the date and criteria of the asthma diagnosis from their medical records to ensure that the diagnosis of asthmatics included in our study fulfilled our criteria. For all cases, we verified from their medical records that they did not have a previous asthma diagnosis. Eligible subjects were invited to participate in the study, and informed consent was asked by their physician or through a letter sent by the National Social Insurance Institution. The cases answered the questionnaire at the time of recruitment. Recruitment of controls took place at regular intervals throughout the study period. Informed consent was requested in the letter and returned in a prepaid envelope to the research nurse of the study project.
Measurement Methods
Questionnaire. The self-administered questionnaire, modified from the Helsinki Office Environment Study questionnaire (24,25) to be used in a general population, included six sections: 1) personal characteristics, 2) health information, 3) active smoking and environmental tobacco smoke exposure, 4) occupation and work environment, 5) home environment, and 6) dietary questions.
Lung function measurements. We applied the same lung function protocol to all patients with suspected asthma. The only exception was patients recruited through the National Social Insurance Institute, for whom we obtained lung function data by abstracting from the medical records.
Baseline spirometry. For all patients with suspected bronchial asthma, we recorded vital capacity and flow-volume curves with a pneumotachygraph spirometer connected to a computer and using a disposable flow transducer (Medikro 905; Medikro Ltd., Kuopio, Finland). We carried out the measurements according to the standards of the American Thoracic Society (26). We judged presence of obstruction using the reference values derived from a Finnish population (27).
Bronchodilation test. After baseline spirometry, all patients received 400 µg of salbutamol (albuterol) with a spacer and performed spirometric flow-volume curves after 10 min.
Peak expiratory flow (PEF) follow-up. All patients performed PEF follow-up for at least 2 weeks with a mini Wright meter. We instructed subjects to carry out measurements twice a day, in the morning and in the evening. During the second week, subjects performed measurements before and 15 min after short-acting bronchodilating medication. Subjects recorded all three readings, and we used the highest value in the analyses.
Steroid treatment response. We recommended that physicians give a 2-week oral steroid treatment to those with a strong suspicion of asthma, if the other diagnostic tests were negative. The patient was asked to perform 2 weeks of PEF follow-up during this treatment, and spirometry was carried out again at the end of this treatment period to judge the response.
Statistical Methods
We used exposure odds ratio (OR) to quantify the relations between exposures and outcome, and estimated adjusted OR in logistic regression analysis. We used the following covariates to adjust for potential confounding: sex, age, parental atopy or asthma, education (as an indicator of socioeconomic status), personal smoking, dampness and mold problems in the home or at work, exposure to environmental tobacco smoke, any history of pets in the home, and self-reported occupational exposure to sensitizers, dusts or fumes (except self-reported exposure to molds).
We studied the independent predictive value of the four exposure indicators (water damage, damp stains, visible mold, and mold odor) in the workplace (for those working at least 50% of their workday indoors) and in the home by including all the exposure indicators as well as covariates in the model. We also elaborated the role of exposure time period by fitting time-specific exposure variables. We combined occurrence of dampness and mold problems during different time periods because we detected no meaningful trends according to the time specificity of exposure (data not shown). We combined any visible mold and/or mold odor in the workplace to represent the main exposure parameter. These two exposure indicators were closely related and had strong overlap, so including them separately in the models was not meaningful. The reference category consisted of those reporting no mold or dampness exposure. We also analyzed the data after excluding patients recruited by the National Social Insurance Institution.
We systematically studied potential modification of the relation between main exposure parameter and risk of asthma by comparing the adjusted ORs by sex, age (20-29, 30-49, and 50-63 years), parental atopy or asthma (yes/no), and smoking (never, former, current).
Finally, we quantified the impact of exposure as an attributable fraction (28) or etiologic fraction (29), providing the fraction of exposed cases for whom the disease is attributable to the exposure (28). We calculated the attributable fraction (AF)
AF = (OR - 1)/OR,
where OR is the adjusted OR due to the exposure of interest, an unbiased estimate of incidence ratio in a population-based case-control study (29). We calculated the 95% confidence interval (CI) using the corresponding interval of OR.
Results
Characteristics and Exposure of Cases and Controls
A larger proportion of cases than controls were women, young, current smokers, and exposed to environmental tobacco smoke and to pets; had lower education; and reported a history of parental allergic diseases (Table 2).

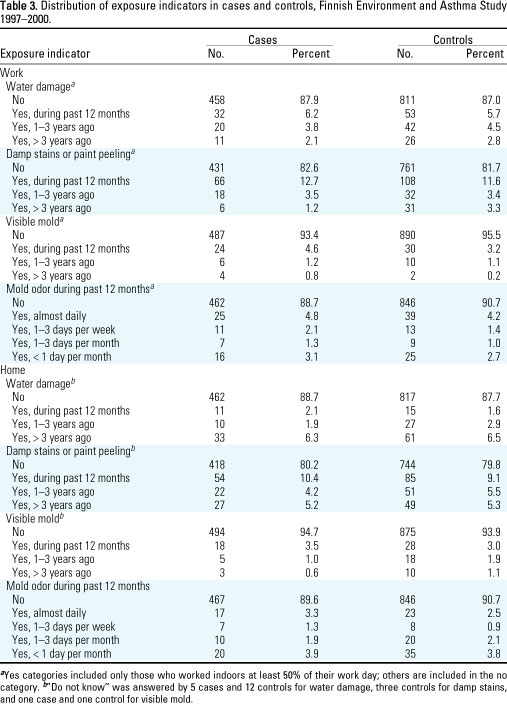
A larger percentage of cases than controls reported presence of visible mold (6.6% vs. 4.5%) and mold odor (11.3% vs. 9.3%) in the workplace (Table 3). The frequency distributions of water damage and damp stains or paint peeling in the workplace and of all the four exposure indicators in the home were similar among cases and controls.
Indoor Dampness Problems and Molds and the Risk of Asthma
The risk of asthma was related to the presence of visible mold and/or mold odor in the workplace, but not to water damage or damp stains alone, as shown in Table 4. The adjusted OR for any exposure to visible mold or mold odor was 1.54 (95% CI, 1.01-2.32). The risk of asthma was related to none of the exposure indicators in the home. The results were essentially similar in the analyses that excluded cases recruited through the National Social Insurance Institution. We estimated the fraction of asthma attributable to workplace mold exposure to be 35.1% (95% CI, 1.0-56.9%) among the exposed.


The relation between workplace mold exposure and the risk of asthma was slightly stronger in women than in men (Table 5). The relation was strongest in the youngest age group and stronger in current smokers than in former smokers or never smokers. The relative risk was essentially similar in those with and without parental atopy.
Discussion
We found a significantly increased risk of new asthma in adults in relation to the presence of visible mold and/or mold odor in the workplace, whereas water damage or damp stains alone were not associated with asthma. The mechanisms by which indoor dampness problems could lead to an increased risk of asthma are not well understood, and several potential causes have been suggested: molds, bacteria, house dust mites, and enhanced emission of chemicals from surface materials (9,15). Our results emphasize the role of molds (and possibly bacteria) as an important cause of asthma, rather than dampness per se. Potential mechanisms by which indoor molds could induce asthma include immunoglobulin E-mediated hypersensitivity reactions, toxic reactions caused by mycotoxins, and nonspecific inflammatory reactions caused by irritative volatile organic compounds produced by microbes or cell wall components, such as 1,3-ß-d-glucan and ergosterol (9,30-32). Different species of molds may induce asthma by different mechanisms, or molds may induce health effects by combined mechanisms (32).
The risk of asthma was not associated with the presence of dampness or molds at home in this study. We have no reason to believe that effects of similar exposures at home and at work would be different. Rather, the difference in effect estimates in our study are likely explained by more extensive mold problems at work than at home. We did not quantify the extent of such problems, but it is likely that in the workplace people do not notice small dampness problems easily, because they change work areas often, and thus more extensive mold growth may develop. In addition, influencing the work environment is often more difficult. At home, people tend to pay attention to water damage and repair it before more advanced mold problems develop, because such damage reduces the value of the property. In 1998 in the Pirkanmaa area, 67% of the population owned the residences in which they lived. Other potential explanations for these differences include, for example, ventilation systems of workplaces favoring the spread of molds and their metabolites into indoor air. The attributable fraction of asthma due to workplace mold was surprisingly high: 35% among the exposed cases.
We found that women, the young, and smokers are especially susceptible to the effects of workplace molds. The mechanisms of such susceptibility are not known and should be studied further. The young and women may have more extensive exposures, because they are often in lower positions in the workplace and therefore have less influence on their work environment. Also, modification of immunologic or other inflammatory reactions may play a role in sensitivity, at least in current smokers.
Validity Issues
We were able to recruit a high proportion of new cases of asthma by a thorough recruitment through the health care system (response rate, 90%) and with the help of the National Social Insurance Institution providing us a route to reach those asthmatics that we missed by our recruitment system (response rate, 78%). The health insurance provided by the National Social Insurance Institution covers the whole Finnish population, and its medication files have practically a full coverage of asthmatics who fulfill the diagnostic criteria required for reimbursement in Finland. The response rate among the control population was also relatively high, especially among those who had a phone number in the Pirkanmaa region and were likely to really live in this area during our study period. Thus, any major selection bias is unlikely in our study.
To reduce information bias, we introduced the study to the participants as a study on environmental factors and asthma in general (the Finnish Environment and Asthma Study), with no special focus on mold and dampness problems. We collected information on exposures in a similar way from cases and controls. The physicians responsible for the diagnostic procedures of asthma were unaware of the questionnaire responses of the study subjects. Our finding of an increased risk of asthma in relation to workplace exposure but not in relation to home exposure supports unbiased reporting; it is unlikely that subjects would associate their symptoms to a specific exposure in one environment but not in the other. In the analyses excluding cases recruited by the National Social Insurance Institution (i.e., some time after their diagnosis was made), the OR related to workplace mold exposure remained increased (1.38) but was slightly reduced. This indicates that some overreporting of workplace exposure may have taken place, but this does not explain the effect entirely. On the other hand, studies comparing self-reported dampness with site visits have usually shown that subjects tend to underestimate their exposures (7,9,11). Thus, self-report of exposures may have led to some underestimation of the risks in our study (e.g., the risks for home exposures). We defined asthma on the basis of objective clinical findings to eliminate information bias concerning the outcome.
We were able to adjust for a number of potential confounders (see "Statistical Methods") in logistic regression analysis to eliminate these factors as potential explanations for our results. We adjusted for parental atopy to control for genetic predisposition, but not for subjects' own atopy, because this may be in the causal pathway for effects of indoor molds.
Synthesis with Previous Knowledge
Earlier studies on indoor dampness and mold problems in adults have been mainly cross-sectional or prevalent case-control studies in design; therefore, our results cannot be compared directly with them. One population-based study from Sweden assessed adult-onset asthma based on questionnaire reports of asthma (20). A significant OR of 2.2 was reported in relation to visible mold at home, whereas visible dampness alone was not significantly related to asthma. The Swedish study assessed the onset of asthma retrospectively based on self-reported information about the year of diagnosis. The subjects had to recall both the year of diagnosis and exposures as far back as 14 years before, which makes the study vulnerable to recall bias. The Swedish study did not adjust for or estimate the risk related to workplace mold problems.
We identified no earlier study that had assessed the relation between workplace dampness and mold problems and the risk of asthma. A previous study in Finnish daycare nurses reported the risk of wheezing related to workplace exposure, while adjusting for home exposure (5). The OR was 1.66 when water damage was present and 1.28 when water damage and mold odor both were present. These estimates are close to our OR of asthma among women (1.67). In addition, three other studies reported risk estimates of wheezing in relation to workplace dampness or mold exposures. A study from the United States reported an OR of 2.8 for usual wheezing and 1.9 for occasional wheezing in association with mold exposure in problem office buildings in Florida (22). A study of Taiwanese daycare centers found an increased risk of wheezing in relation to stuffy odor (OR, 1.38), visible mold (OR, 1.39), and water damage (OR, 1.32) (21). Another Taiwanese study of office workers found similar ORs for chest tightness and chest pain (10).
Two Dutch studies assessed the risk of asthma related to residential dampness stratified by sex. In one of them (18) the risk was similar in men (OR, 1.29) and women (OR, 1.25), whereas the other (13) found, in agreement with our study, a greater risk in women (OR, 4.16) than in men (OR, 1.15). The Swedish study (20) found an essentially similar risk of asthma related to visible mold growth among men (2.7) and women (2.0). Modification by age, genetic predisposition, or smoking status has not been previously studied.
Conclusion
The present results provide new evidence of the relation between workplace exposure to indoor molds and development of asthma in adulthood. Our findings suggest that indoor mold problems constitute an important occupational health hazard.
References and Notes
1. Platt SD, Martin CJ, Hunt SM, Lweis CW. Damp housing, mould growth, and symptomatic health state. Br Med J 298:1673-1678 (1989).
2. Dales RE, Zwanenburg H, Burnett R, Franklin CA. Respiratory health effects of home dampness and molds among Canadian children. Am J Epidemiol 134:196-203 (1991).
3. Brunekreef B. Associations between questionnaire reports of home dampness and childhood respiratory symptoms. Sci Total Environ 127:79-89 (1992).
4. Jaakkola JJK, Jaakkola N, Ruotsalainen R. Home dampness and molds as determinants of respiratory symptoms and asthma in pre-school children. J Exp Anal Environ Epidemiol 3:129-142 (1993).
5. Ruotsalainen R, Jaakkola N, Jaakkola JJK. Dampness and molds in day-care centers as an occupational health problem. Int Arch Occup Environ Health 66:369-374 (1995).
6. Maier WC, Arrighi HM, Morray B, Llewellyn C, Redding GJ. Indoor risk factors for asthma and wheezing among Seattle school children. Environ Health Perspect 105:208-214 (1997).
7. Williamson IJ, Martin CJ, McGill G, Monie RDH, Fennerty AG. Damp housing and asthma: a case-control study. Thorax 52:229-234 (1997).
8. Nafstad P, Øie L, Mehl R, Gaarder PI, Lødrup-Carlsen KC, Botten G, Magnus P, Jaakkola JJK. Residential dampness problems and symptoms and signs of bronchial obstruction in young Norwegian children. Am J Respir Crit Care Med 157:410-414 (1998).
9. Norbäck D, Björnsson E, Janson C, Palmgren U, Boman G. Current asthma and biochemical signs of inflammation in relation to building dampness in dwellings. Int J Tuberc Lung Dis 3:368-376 (1999).
10. Wan G-H, Li C-S. Dampness and airway inflammation and systemic symptoms in office building workers. Arch Environ Health 54:58-63 (1999).
11. Nevalainen A, Partanen P, Jääskeläinen E, Hyvärinen A, Koskinen O, Meklin T, Vahteristo M, Koivisto J, Husman T. Prevalence of moisture problems in Finnish houses. Indoor Air Suppl 4:45-49 (1998).
12. Brunekreef B, Dockery DW, Speizer FE, Ware JH, Spengler JD, Ferris BG. Home dampness and respiratory morbidity in children. Am Rev Respir Dis 140:1363-1367 (1989).
13. Waegemaekers M, Van Wageningen N, Brunekreef B, Boleij JSM. Respiratory symptoms in damp houses. A pilot study. Allergy 44:192-198 (1989).
14. Spengler JD, Neas L, Dockery DW, Speizer F, Ware J, Raizanne M. Respiratory symptoms and housing characteristics. Indoor Air 4:72-82 (1994).
15. Bornehag C-G, Blomquist G, Gyntelberg F, Järvholm B, Malmberg P, Nordvall L, Nielsen A, Pershagen G, Sundell J. Dampness in buildings and health. Nordic interdisciplinary review of the scientific evidence on associations between exposure to dampness in buildings and health effects (NORDDAMP). Indoor Air 11:72-86 (2001).
16. Hyndman SJ. Housing dampness and health amongst British Bengalis in East London. Soc Sci Med 30:131-141 (1990).
17. Dales RE, Burnett R, Zwanenburg H. Adverse health effects among adults exposed to home dampness and molds. Am Rev Respir Dis 143:505-509 (1991).
18. Brunekreef B. Damp housing and adult respiratory symptoms. Allergy 47:498-502 (1992).
19. Hu FB, Persky V, Flay BR, Richardson J. An epidemiological study of asthma prevalence and related factors among young adults. J Asthma 34:67-76 (1997).
20. Thorn J, Brisman J, Torén K. Adult-onset asthma is associated with self-reported mold or environmental tobacco smoke exposures in the home. Allergy 56:287-292 (2001).
21. Li C-S, Hsu C-W, Lu C-H. Dampness and respiratory symptoms among workers in daycare centers in a subtropical climate. Arch Environ Health 52:68-71 (1997).
22. Hodgson MJ, Morey P, Leung W-Y, Morrow L, Miller D, Jarvis BB, Robbins H, Halsey JF, Storey E. Building-associated pulmonary disease from exposure to Starchybotrus chartatum and Aspergillus versicolor. J Occup Environ Med 40:241-249 (1998).
23. Committee on National Asthma Program in Finland. Asthma Program 1994-2004 [in Finnish]. Report No. 16. Helsinki:Ministry of Social Affairs and Health Publications, 1994.
24. Jaakkola JJK, Miettinen P. Type of ventilation system in office buildings and sick building syndrome. Am J Epidemiol 141:755-765 (1995).
25. Jaakkola MS, Jaakkola JJK. Office equipment and supplies: a modern occupational health concern? Am J Epidemiol 150:1223-1228 (1999).
26. American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med 152:1107-1136 (1995).
27. Viljanen AA, Halttunen PK, Kreus K-E, Viljanen BC. Spirometric studies in nonsmoking, healthy adults. Scand J Clin Lab Invest 42(suppl 159):5-20 (1982).
28. Greenland S. Applications of stratified analysis methods. In: Modern epidemiology (Rothman KJ, Greenland S, eds). 2nd ed. Philadelphia:Lippincott-Raven, 1998;295-297.
29. Miettinen OS. Proportion of disease caused or prevented by a given exposure, trait or intervention. Am J Epidemiol 99:325-332 (1974).
30. Husman T. Health effects of indoor-air microorganisms. Scand J Work Environ Health 22:5-13 (1996).
31. Thorn J, Rylander R. Airways inflammation and glucan in a rowhouse area. Am J Respir Crit Care Med 157:1798-1803 (1998).
32. Johanning E, Landsbergis P, Gareis M, Yang CS, Olmsted E. Clinical experience and results of a sentinel health investigation related to indoor fungal exposure. Environ Health Perspect 107(suppl 3):489-494 (1999).
Last Updated: April 4, 2002